Treated conditions
Home » Areas of expertise » Acoustic Neuroma
Treated conditions
Acoustic Neuroma
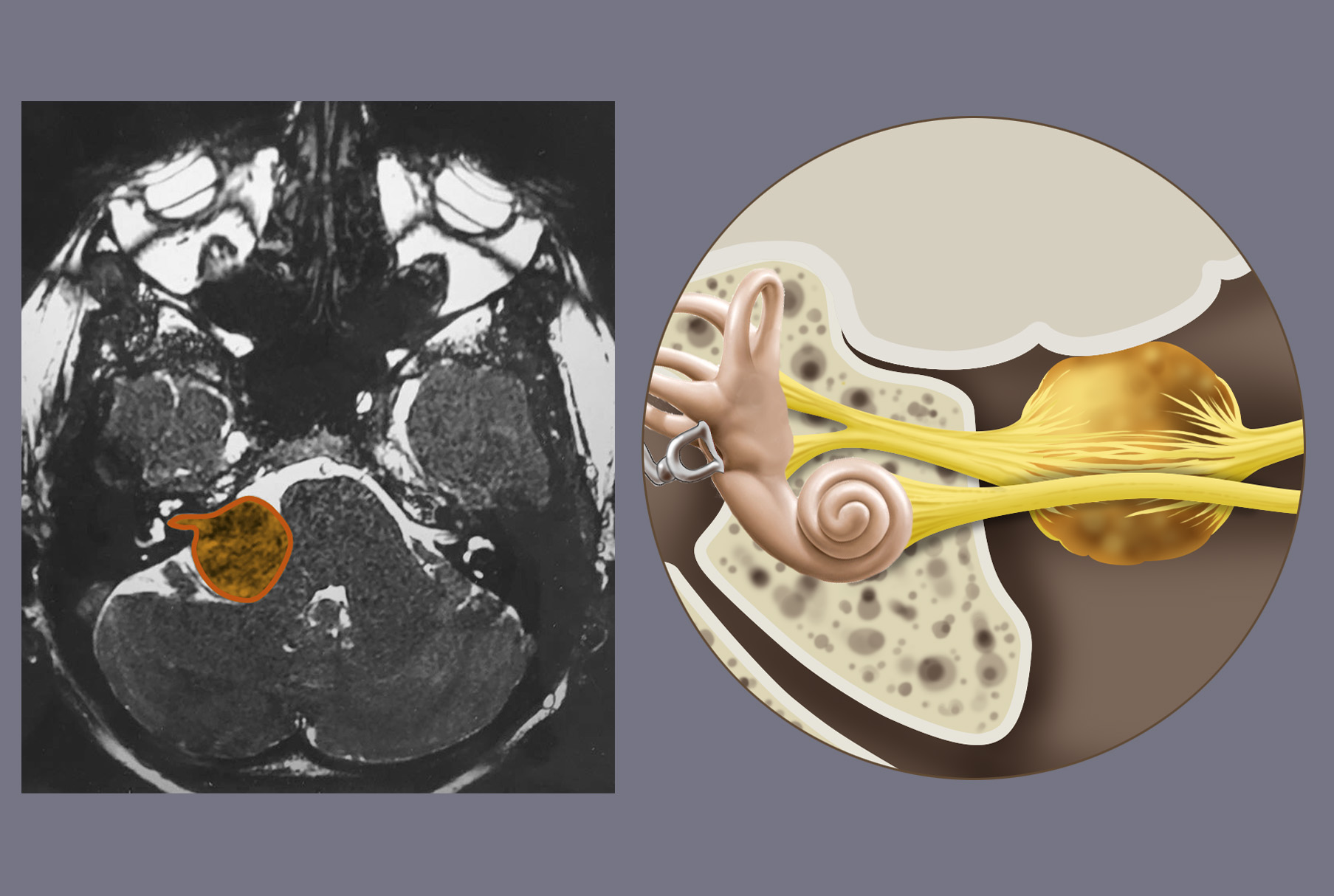
The acoustic neuroma (or vestibular Schwannoma) is a benign slow-growing tumor originating from the Schwann cells of the vestibular nerve in the internal auditory meatus from where it spreads to the cerebellopontine angle.
It represents 7-8% of all intracranial tumors.
95% of acoustic neuromas are unilateral, but in cases of type 1 or type 2 neurofibromatosis, it may be bilateral or associated with other lesions.
Symptoms
Due to the location of the tumor, the initial symptoms are caused by the compression of the acoustic-vestibular nerve and include:
- progressive loss of hearing
- tinnitus
- dizziness
- balance disorders
When the tumor increases in size and starts to occupy the cerebello-pontine angle, consequently compressing other cranial nerves (such as the trigeminal and facial ones), the cerebellum, and the brainstem, other symptoms may arise, such as:
- headache
- facial paraesthesia (sensory disorder or numbness)
- facial paresis (muscle disorders)
- diplopia (double vision)
- ataxia (coordination disorder)
- dysmetria (alteration of the measure of voluntary movements)
- nausea
- vomiting
Should the neuroma reach a significant size, it may hinder the free circulation of fluids and lead to hydrocephalus as well as to an increase in intracranial pressure.
Diagnosis
Diagnosis can be reached by means of brain MRI in which the lesions appear rounded and contrast-enhanced. A brain CT can complement the diagnosis to assess the expansion of the internal auditory meatus.
It is important to complete the diagnosis with functional tests to assess hearing (audiometric testing) and the functionality of the facial nerve (House-Brackmann Classification).
These tests are also useful for a later comparison between the pre- and post-operative patient status.
Treatment
A small and asymptomatic neuroma does not need immediate intervention and can be kept under control with radiological follow-ups.
In general, microsurgical procedures are performed on tumors with a diameter of more than 3 cm or a smaller diameter in young patients with unimpaired hearing.
The possibility of preserving hearing and the integrity of the facial nerve depends on the size of the tumor.
An alternative therapeutic option to surgery is stereotactic radiosurgery (Gamma-Knife), where a beam of radiation is directed to the tumor. It does not require any invasive maneuver and implies only a minor risk of damaging the neural structures.
Radiosurgery is indicated for tumors smaller than 3 cm in diameter and/or for patients with a high anaesthetic risk. It may also be used to treat possible residual tumor of large-size neuromas in case of partial surgical resection in order to preserve the facial nerve.
The acoustic neuroma is a benign slow growing tumor. Therefore, total removal is curative in most cases.